Most common congenital anomalies are PUJO, Hypospadias, Vesico ureteric Reflux and Undescended testis.
Ureteropelvic Junction (UPJ) Obstruction in Children
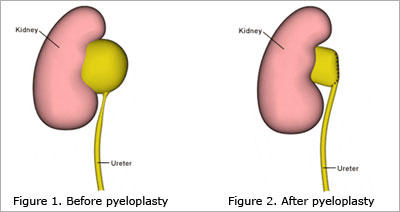
The urine must drain from the kidney through an internal collecting system that ends in a funnel-shaped structure called the renal pelvis and into a natural tube called the ureter. The junction between the renal pelvis and the Ureter is called the pelviuretric junction. Obstruction at this junction is called pelviureteric junction obstruction (PUJO). This is the most common cause of obstruction (blockage) in the urinary tract in children and it is a congenital obstruction. This problem occurs in approximately one in 1,500 children.
Symptoms of UPJ obstruction may be an abdominal mass; a urinary tract infection with fever; flank pain, especially with increased fluid intake; stones and bloody urine.
Diagnosis:
Although ultrasound is a very useful screening test, it is not diagnostic of UPJ obstruction. Intravenous pyelogram/CT urogram/ DTPA renogram are used for diagnosis of PUJ obstruction.
Treatment
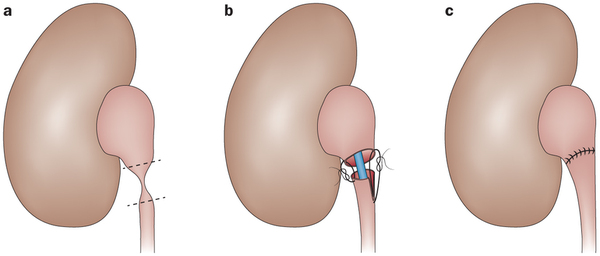
The classic treatment of UPJ obstruction is an operation to remove the abnormal PUJ and to reattach the ureter to the pelvis of the kidney, creating a wide junction between the two. This operation, called a pyeloplasty, allows rapid and easy drainage of urine produced by the kidney and relieves symptoms and the risk of infection. The incision usually is just below the ribs and just behind a line that would pass from the patient's arm to the leg on the affected side. The incision usually is two to three inches long. Traditionally this was done through open surgery, but in recent years with the evolution of key hole surgery it is routinely done with the minimally invasive technique.
Hypospadias
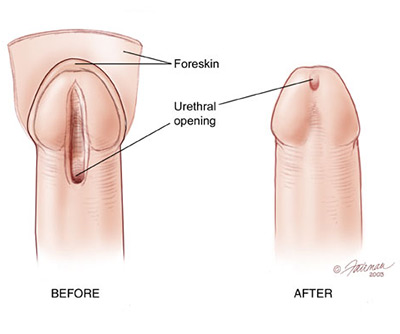
Hypospadias is a condition in which the urethral opening at the end of the penis is not where it should be. Instead of ending at the tip of the penis, the urethral opening opens at the undersurface at the head of the penis or along the shaft of the penis. In more rare cases, the urethral opening is located on the scrotum or at the perineum, the area between the scrotum and the anus. Additionally, the foreskin does not usually completely wrap around the head of the penis and, occasionally, a curvature of the penis, called a chordee, can be present. Hypospadias is a congenital defect, meaning that it occurs before birth.
How is Hypospadias Diagnosed?
Hypospadias is most often noticed at birth. Not only is the meatus in the wrong place, but the foreskin is often not completely formed on its underside. This results in a "dorsal hood" that leaves the tip of the penis exposed.
How is Hypospadias treated?
The goal of any type of hypospadias surgery is to make a normal, straight penis with a urinary channel that ends at or near the tip.
The operation mostly involves 4 steps:
• Straightening the shaft
• Making the urinary channel
• Positioning the meatus in the head of the penis
• Circumcising or reconstructing the foreskin
In some cases the repair is done in stages. These are often proximal cases with severe chordee. Surgeons prefer to do hypospadias surgery in full-term and otherwise healthy boys between the ages of 6 and 12 months.
Vesico Ureteral Reflux
Urine normally flows in one direction down from the kidneys through tubes called ureters, to the bladder. Vesicoureteral reflux (VUR) is the condition in which urine travels backward from the bladder toward the kidney and may affect one or both ureters and then the kidneys. About one-third of children with urinary tract infections are found to have vesicoureteral reflux (VUR). In most children, reflux is a birth defect and is caused by an abnormal attachment between the ureter and bladder with a short, ineffective flap valve. In some children, an infrequent urination pattern may cause reflux to occur. When the "flap valve" malfunctions and allows urine to flow backward, bacteria from the bladder easily enters the kidney. A child with reflux is more likely to develop a kidney infection (pyelonephritis) that can cause kidney damage. When urine backflow is more severe, the ureters and kidneys become large and distorted. More severe reflux is associated with greater kidney damage in the presence of infection.
How is vesicoureteral reflux (VUR) diagnosed?
Reflux is diagnosed with a xray of the bladder called a voiding cystourethrogram (VCUG). A thin plastic tube called a catheter is inserted into the urethra. Fluid containing an X-ray dye is injected through the tube until the bladder is full, and then the child is asked to urinate. Pictures of the bladder are taken to see if the dye goes backward up to one or both kidneys. If reflux is found, an isotope renal scan may be done to check how well the kidneys are working and to look for kidney damage.

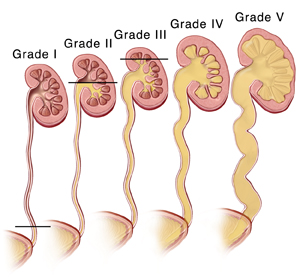
Grades of vesicoureteral reflux (VUR):
The most common system of grading reflux - the International Study Classification - includes five grades.
Grade I - results in urine reflux in to the ureter only.
Grade II - results in urine reflux into the ureter and the renal pelvis, without distention (hydronephrosis).
Grade III - results in reflux into the ureter and the renal pelvis, causing mild hydronephrosis.
Grade IV - results in moderate hydronephrosis.
Grade V - results in severe hydronephrosis and twisting of the ureter.
What are the risks of vesicoureteral reflux (VUR)?
In children with reflux and UTI, kidney damage may occur. Higher grades of reflux are associated with greater risk of kidney damage.
How is vesicoureteral reflux (VUR) treated?
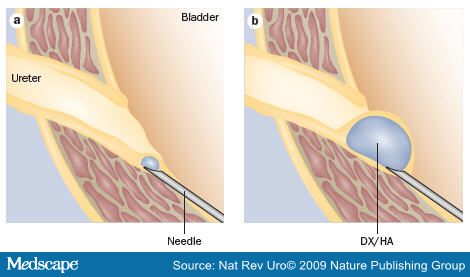
Children with reflux undergo a careful urological history and physical exam to determine the level of risk for developing kidney damage or scarring. The basis for medical treatment is that reflux often will gradually disappear. The average age for this to occur is five to six years. The goal of medical treatment is to prevent UTI and kidney damage while growth and development allow reflux to disappear with time. The goal of surgical treatment is to cure reflux with an operation and thus avoid the potential risks of continued reflux. The usual type of surgical therapy is performed under general anesthesia through an incision in the lower abdomen. The operation consists of correcting the flap-valve attachment to the ureter to the bladder to prevent reflux from occurring. After the operation, a follow-up X-ray evaluation is performed several months later to be certain that the operation was successful. Once the reflux is successfully corrected, it is unlikely to recur. Another type of surgical correction is called endoscopic surgery. The surgeon inserts an instrument called a cystoscope into the urethral opening to see inside the bladder. A substance is then injected into the area where the ureter enters the bladder to try to repair the reflux.
Undescended Testicles (Cryptorchidism)
Normal testicles form early in a baby boy's growth. They form in the lower belly (abdomen), but descend, or "drop," into the scrotum toward the end of pregnancy. Normal testicles attach themselves with stretchable tissue in the bottom of the scrotum. This is controlled by the baby's normal hormones.
What are Undescended Testicles?
An undescended testicle (or "testis") is when it fails to drop into the normal place in the scrotum. This issue is found in about 3 or 4 out of 100 newborns (and up to 21 out of 100 premature newborns). Luckily, about half of these testicles will drop on their own during the first 3 months of life. But testicles won't drop on their own after 3 months of age. Thus, about 1 or 2 out of 100 boys with undescended testicles will need treatment. The testicles need to be 2 to 3 degrees cooler than normal body temperature to make sperm. The scrotum is many degrees cooler than body temperature, and so is the ideal place for the testicle. Testicles that don't drop into the scrotum won't work normally. The longer the testicles are too warm, the lower chances are that the sperm in that testicle will mature normally. This can be a cause of infertility, especially when both testicles are affected.
Undescended testicles are also linked to a higher risk of:
Testicular cancer in adulthood (though the risk is still less than 1 in 100)
Testicular torsion (twisting of the chord that brings blood to the scrotum)
Developing a hernia near the groin
In most children with this health issue, it's not known why the testicles fail to drop. It may be because the testicles aren't normal to start with. In other cases, there's a mechanical problem. The testicles drop but miss the scrotum, ending up next to the scrotum instead. These are called "ectopic testicles." Or it may be that the baby's hormones can't stimulate the testicles normally. No studies have shown that the problem is caused by something the mother did or ate during pregnancy.
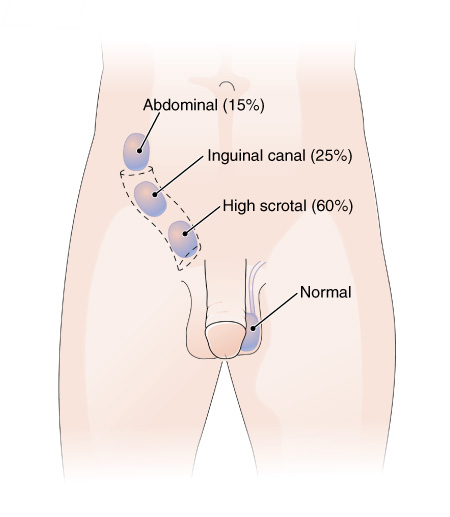
How are Undescended Testicles Diagnosed?
A testicle that can't be felt in a physical exam is called "nonpalpable." Nonpalpable testicles may be in the abdomen (undescended), absent, or very small ("atrophic"). It's important to find out whether there is a testicle that hasn't dropped. An undescended testicle left inside the abdomen could form a tumor later in life. Such a tumor might not be noticed until it becomes quite large or causes symptoms. Unfortunately, there's no test, such as an ultrasound, that can definitively show whether a testicle is there. Surgery is the only way to find out for sure.
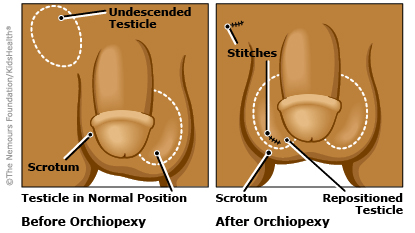
How are Undescended Testicles Treated?
The testicle won't drop after 3 months of age, so the only treatment choice is surgery. The timing takes into account when the child is able to handle anesthesia and the surgery.
This surgery is called an orchiopexy. The child is put under (general anesthesia) for this surgery. A cut about 1 inch long is made in the groin area (most often it can hardly be seen later). The testicles are freed from all nearby tissues so that it moves easily into the scrotum. Then it is stitched into place.